Madhab K. Chattopadhyay
Introduction All of us (barring the exception of a fortunate few) have to seek medical treatment of various health problems during different phases of life. So problems related to medical treatment impact us in various ways. This article deals with two major problems that are widely talked about at present among the medical practitioners, policy-makers and common people alike.
1. Quackery The term “Quackery” implies false claims to have special knowledge in a field. This discourse is focused on therapeutics and quackery in this article means clinical practice as a doctor without having a requisite qualification. Fraudulent medical practitioners, who claim to be doctors without studying in a recognized medical college, are rampant in India and some other third world countries. Most of them claim to be allopath since we generally resort to allopathic treatment when we fall ill. Following a crackdown of police on quacks in West Bengal, it was revealed that some of these self-appointed doctors had degree in pure science (e.g, B.Sc with physics, chemistry or biology), some had a diploma in homeopathy (mostly earned through a correspondence course run by a unrecognized organization) while some had passed only Higher Secondary Examination conducted by the West Bengal Board. How did they venture into the area of medical practice? Some of them had experience of working as a compounder (not as a registered pharmacist) at the chamber of a doctor or at the dispensary of a hospital. Some of them were selling medicines a shop. Some others trained themselves simply by going through some Bengali books on allopathic medicines which are freely available in the market. Needless to say, common people by and large, do not bother to verify the educational background of the doctor while approaching him for medical treatment. The symptom-based prescriptions of these fake doctors provide temporary relief to the patients. But this practice is associated with serious risks. The quacks, not having any in-depth knowledge about drugs and their side-effects, may endanger the life of the patient. When the patient approaches a trained medical practitioner not having any relief by the treatment of the quack, he finds it difficult to choose the correct medicine since in most of the cases he cannot get any idea as to which drugs were applied to the patient by the quack. Suppression of the symptoms by the symptom-based approach of the quack may also complicate the diagnosis.
Suggested remedial measures: Pros and cons
1.1.1 Legal action against the quacks Quite reasonably, people from different walks of life, are condemning such malpractice in strongest possible terms and urging the government to locate the wrong-doers and bring them to the book. They are demanding exemplary punishment of the quacks to put an end to their business. Unfortunately a sizeable fraction of the urban population (including also the educated denizens) promotes quackery in various ways. When they fall ill, instead of seeking help from a qualified doctor, they approach a local pharmacy. The shop-keeper gives them some medicines based on the symptoms. The dual role played by him as a doctor and as a pharmacist promotes sale in his business. His patient cum customer also feels happy to bypass the doctor since it saves a lot of time and money. The role of the pharmacist as a doctor becomes more prominent (and sometimes indispensible) in the rural areas where qualified doctors are seldom available. If the police initiate legal action against the quackery of a pharmacist, who is seeing patients and selling medicines to the patients in a remote village, they are likely to face stiff resistance from the local people. While the attitude of the people appears to be tenable in view of the dismal state of healthcare system in rural India, it is hardly possible to justify similar attitude of the urban people who, despite having the means and scope to approach a qualified doctor, prefer to depend upon the medicines prescribed and dispensed by the pharmacist.
1.1.2 Increase in the number of doctors
Many people believe that we can put an end to quackery by setting up more medical colleges and thereby generating more doctors. The idea is not tenable for various reasons.
1.1.2.1 Challenging dimension of the task
First of all, let us examine the feasibility of implementing the idea. The standard of medical care in a country can be adjudicated, at least to some extent, by the number of doctors available for every 1000 people. Based on a report, provided by the Medical Council of India (MCI), Smt. Anupriya Patel, Minister of State for Health, informed Lok Sabha on 21 July 2017 that less than one doctor was available for 1000 people in India. The Doctor : Patient ration in this country was only 0.62, that was far below the ratio 1: 1000, recommended by the World Health Organization (WHO). The ratio is 4.125:1000 for Germany, 3.374 :1000 for Russia, 3.306:1000 for Australia, 3.227:1000 for France, 2.554 :1000 for the US,1.852 : 1000 for Brazil, 1.49: 1000 for China, , 0.806 : 1000 for Pakistan’ 0.334:, 1000 for Afghanistan and 0.309 : 1000 for Bangladesh. Hence, notwithstanding the fact that India is the largest producer of doctors in the world (49840 seats in 370 medical colleges compared to 18000 doctors produced per year in the US, https://thewire.in/education/medical-colleges-mci-mbbs ), we require to double the number of seats right now to reach the Doctor : Patient ratio recommended by the WHO. The government does not have the resource to meet the challenge. Hence, private organizations have to be granted permission in a very large scale to open medical colleges. But it will be difficult to maintain standard and quality of education and training in those colleges. The newly opened colleges may not survive the stringent quality control system of the Medical Council of India (MCI). “The proposed massive expansion, which would reduce the medical colleges to pathshalas (primary schools), is ill advised.” observes Dr M.G.Deo, the noted oncologist, pathologist and educationist.“ He believes that the idea “will not solve India’s woes of poor health services, but only downgrade country’s standing in the medical world.”
1.1.2.2 Doubtful link between number of doctors and standard of medical care
“Is it really possible to improve the standard of medical care in a country simply by increasing the number of doctors?”- this thought-provoking question was pursued by a group of researchers at the Centre for Health Services and Policy Research in the University of British Columbia (Vancouver, Canada). The Organization for Economic Cooperation and Development (OECD) is an international society formed in 1961 to promote economic development and world trade. Some of the members include the US, the UK, Germany, France, Belgium, Spain, Norway, Turkey, Japan, Australia and New Zealand. In January 2008, the Canadian Medical Association (CMA) launched a ‘More doctor More care” campaign. At that time 26000 more doctors were needed in Canada to meet the average Doctor : Population ratio of the OECD countries. It was at that juncture when the researchers at the aforementioned institute addressed the question whether or not the number of doctors was the right or a relevant parameter for the standard of healthcare. Avoidable mortality, which means extent of preventable death (death before the age of 75) from causes ( e.g bacterial infections, influenza, epilepsy, treatable cancers, maternal death, complications from common surgical procedures) that could be avoidable by timely and effective healthcare, is considered a valid indicator to assess the standard of medical care in a country. Analyzing data obtained from 19 OECD countries, they did not find any association between overall supply of physicians and avoidable mortality. The investigators also did not find any association between avoidable mortality and some other parameters e.g general practitioners per capita, family physicians per capita, specialists per capita, nurses per capita, doctors and nurses per capita and health expenditures per capita. Thus, even if we could increase the supply of qualified physicians, we may not achieve an improved healthcare system.
1.1.3 Production of rural medical personnel by short-term training
Scarcity of qualified doctors and lack of proper infrastructure for medical treatment in the villages pose a serious challenge to the rural healthcare system. Because of the non-availability of the qualified medical practitioners, the villagers are compelled to dependent upon the illegal practice of the pharmacists and also on the service of the village doctors, having no formal education or training in medicine. Seeing no scope of improvement of the situation in the near future, the West Bengal (WB) Government is mooting the idea of providing training to some of the village doctors so that they could take care of the health problems of the villagers to some extent and timely refer them to a qualified medical practitioner or hospital. Earlier a proposal was raised to reintroduce the Licentiate in Medical Faculty (LMF) course in WB. The LMF curriculum was started in British India to meet the crying need of qualified medical personnel in the northeastern region of the country. It was continued till 1962. But when the WB government thought of reviving it to meet the shortage of doctors in the 1980s, it was strongly opposed by the doctors, who were dead against the idea. They argued that it would be unfair to leave the life of the villagers in the hand of some unqualified and untrained persons who claim to be doctors. Their concern about the rural people, though sounding fully justified, was mocked at by a section of the villagers, who found it ridiculous that the doctors who did not want to serve the villagers, were getting worried about them. They wholeheartedly supported the proposal of the government emphasizing that instead of dying helplessly, they would prefer to get at least some amount of medical care from the trained village doctors. However the proposal was not actualized for various reasons. Now the present WB government is considering the proposal again.
1.1.3.1 Barefoot doctors
The idea of generating some village doctors by providing training to some local people, who are working as doctors without studying in any medical college, is neither new nor anything outlandish. A similar idea was implemented in China during the second half of the last century. Usually students who passed from the secondary schools were chosen for the program. They were trained in a hospital (usually for six months) on prevention of epidemics, treatment of diseases that were generally found to affect the villagers and use of some Western medicines and techniques. Qualified doctors were also sent to the villages to train these “barefoot doctors”. The trainees were generally farmers and while receiving the training, they were allowed to do their work in their farms. About one fifth of them later on joined the medical college. The scheme was successful in providing health care in the rural areas in an affordable cost and it earned accolade from WHO as a “successful example of solving shortages or medical services in rural areas”. The potential of a multi-topic medical training as an effective short-run strategy to improve healthcare in India was also demonstrated in a study (published in the premier journal Science) led by Dr Abhijit V.Banerjee, a Ford Foundation International Professor of Economics at MIT, US. Hence, though it may appear paradoxical that the WB government is arresting and punishing the quacks in the urban area and at the same time launching a scheme of producing some village doctors who are nothing more than quacks, the utility of the scheme cannot be winked at. The trained health workers will be forbidden to claim that they are doctors and also debarred from writing “Dr” before their name. The WB government believes that if they are trained, they can no longer be called quacks. After getting registered as community health workers, they will be more accountable and hence if any one of them violates the defined limit of his job (i.e, if he prescribes medicines that he is not supposed to use or performs surgery) he could be easily tracked and punished. Thus, it will be possible to minimize indiscriminate quackery of some people, who have no accountability.
1.1.4 Deregulation of the prescriptive right.
The issue of prescriptive right (the legal right to write a prescription) needs serious attention and reconsideration in the Indian perspective. In this country, the right is exclusively confined among the registered medical practitioners, who cry foul whenever any proposal is raised for deregulation of the right. But in the US, the right is deregulated to some extent. According to the law of some states, nurses and advanced practice nurse practitioners have the power to write prescriptions. Veterinarians and dentists also have prescriptive power in all the 50 states. Even clinical pharmacists are given the authority within some defined limitations to write prescriptions in some states. There is another type of health workers called Licensed Physician Assistants in the US. They are meant for prevention and treatment of human illness and injury by working under a supervising physician. Following extensive clinical training, similar to the training of the medical students but shorter in duration, they are licensed to work in hospitals, clinics and other types of healthcare facilities. They are also authorized to write prescriptions within some limitations, defined by the law of different states. Physician Assistants are found also in Canada and known by the designation Physician Associates in the UK. Similar program is undertaken in Australia and New Zealand to help the rural healthcare system.
1.1.5 Scarcity of doctors: A real problem or an overblown issue?
However, some of the doctors believe that the issue of scarcity of allopathic doctors in India is blown out of proportion. The major problem, as perceived and presented by them, is not the shortage of qualified medical personnel but non-recruitment of qualified doctors and lack of infrastructure to retain them in the rural areas. They emphasize that ultimately the pharmaceutical industries and not the common people will be the gainer from deregulation of allopathic prescriptions. Rampant corruption in the health sector leading to the misuse of the allotted funds is also cited as a cause of the miserable state of rural healthcare in this country. According to a recent estimate, India has already achieved a ratio of 1.34 : 1000 Doctor :Patient ratio if the total numbers of available MBBS doctors and ayurvedic doctors are combined. It is also forecast that we shall achieve the WHO recommended ratio of 1: 1000 ratio only with the MBBS doctors a year before the 75th anniversary of Indian independence.
2. Crosspathy
The term crosspathy implies that a physician is prescribing a medicine that is used by the doctors of some other branch of therapeutics Prescription of an ayurvedic medicine by an allopathic doctor or prescription of an allopathic medicine by a homeopathic doctors are some of the example of crosspathy. During the recent past, examples of crosspathy are widely observed in various branches of therapeutics. Analysis of 300 prescriptions collected from the outpatient department of one tertiary care allopathic hospital and same number of prescriptions obtained from the outpatient department of one tertiary care ayurvedic hospital in the urban North India during August to November 2005, revealed that prescription from the allopathic hospital contained 12% ayurvedic drugs (analgesic ointments, liver tonics, drugs for dysfunctional uterine bleeding) and prescriptions from the ayurvedic hospital contained 88% allopathic drugs including non-steroidal anti-inflammartory drugs (22%) and antibiotics (20%). According to a study conducted at the KIM Hospital Mumbai, 975 of the resident doctors did not learn the basics of ayurveda but 67% of them prescribed ayurvedic medicines (e.g, Liv-52, Shatavari, Cystone).The homeopaths also are found to prescribe allopathic medicines in many cases. 2.1 The controversy Crosspathy is not a recent phenomenon. During the 1960s and 1970s, the allopaths were frequently found to prescribe Liv-52 for liver disorder or Antibactrin for boil. It did not occur to anybody that they were crossing their limit. The problematic nature of the practice came to the forefront when the ayurvedic doctors and the homeopaths started prescribing antibiotics and other allopathic drugs in a wide scale. The allopaths argued that use of these drugs are associated with dangerous side-effects, that doctors of other branches of the therapeutics are blissfully unaware of. So the widespread practice of crosspathy is posing a serious threat to the life of the patients. They demanded stringent legal measures to stop crosspathy. The ayurvedic doctors on the other hand pointed out that the allopaths also are resorting to crosspathy by prescribing ayurvedic medicines. They have no formal training about the use of these plant-based medicines. So, similar type of risk is associated also with the crosspathy practiced by them.
2.2 Opinion of the judiciary 2.2.1 Poonam Verma Vs Ashwin Patel and Others case (1996)
The raging controversy has reached the level of judicial intervention. The most famous and widely- cited example in this context was the Smt Poonam Verma vs Ashwin Patel and Others case at the Supreme Court (1996). Smt Verma’s husband Mr Pramod Verma died at the Hinduja Hospital, Mumbai on 14 July 1992, after four and a half hours of admission in an unconscious condition. He was treated for fever on 4 July by Dr Ashwin Patel, a registered homeopath, who prescribed to him some allopathic medicines (including antibiotics) for viral fever and later on for typhoid. When condition of the patient was not improved, he was admitted to a private nursing home (meant for allopathic treatment) on 12 July following the advice of Dr Patel. His condition deteriorated further and he was shifted to the Hinduja Hospital in the evening of 14July. Mrs Poonam Verma lodged a complaint of carelessness and negligence in the treatment of her husband against Dr Patel and the physician of the nursing home to the National Consumer Disputes Redressal Commission (in short Commission), seeking compensation for the damage caused to her. She alleged that Dr Patel administered antibiotics to her husband first for vial fever and subsequently for typhoid without confirming the diagnosis by pathological examinations. Further, he applied allopathic medicines to her husband despite not being authorized to use allopathic medicines. It was his lack of expertise in the practice of allopathic medicine that was responsible for the improper treatment. Her allegation against the physician of the nursing home was that Mr Verma, after admission to the nursing home, was put on intravenous infusion of glucose without being checking for his blood sugar level. She considered it responsible for further deterioration of the condition of her husband.
During the hearing of the case at the Commission , Dr Ashwin Patel informed that he successfully completed a 4-years course on homeopathic medicine and surgery at a homeopathic medical college in Anand (Gujarat) and got registered as a medical practitioner in the states of Gujarat and Maharashtra in 1983. The course completed by him was an integrated curriculum of medicine in both homeopathy and allopathic system of medicine. He admitted to practice both homeopathy and allopathy, which was permitted in Gujarat but he was not aware whether or not it was permitted in Maharashtra. He also informed that in the final year of his study, he attended a training program for 6 months at the Anand Municipal Hospital and another private nursing home at Anand. He further claimed to have experience of working as the Chief Medical Officer at a hospital in Mumbai. Hence the allegation of Mrs Verma that he was not competent to use allopathic medicines was baseless. Prior to July 1992, he was the house physician of Mr Pramod Verma and his family and they used allopathic medicines prescribed by him. He further claimed that he advised the patient to get some pathological tests done, but he did not do so.
The Commission dismissed the case. Smt Verma approached the Supreme Court challenging the judgment delivered by the Commission. In its historical judgment, the apex court made it clear that according to the Bombay Homeopathic Practitioners Act, 1959; the Indian Medical Council Act, 1956 and the Maharashtra Medical Council Act, 1965 a person registered under the Bombay Homeopathic Practitioners Act 1959 can practice homeopathy only and a person having qualification appended to the Indian Medical Council Act, 1956 or the Maharashtra Medical Council Act, 1965 cannot be registered as a Medical Practitioner under the Bombay Homeopathic Practitioners Act, 1959. Briefly speaking, a person registered with one particular system of therapeutics cannot practice in any other branch of therapeutics. It was also underscored that though study of human physiology and anatomy is common in all systems of medicines, study of pharmacology is entirely different in different systems of medicines. In order to examine the validity of allegation of Mrs Verma of negligence in the treatment of her husband also against the physician of the nursing home, the Supreme Court requested the director of the All Indian Institute of Medical Sciences to form a committee of experts in different branches of medicine and to seek their opinion on the treatment of Mr Patel. Following examination of all the relevant documents, the members of the committee could not arrive at a conclusion on the nature of the medical problem Mr Verma was suffering from, since the patient died before a definitive diagnosis could be established. But they found the treatment done at the nursing home and the hospital in keeping with the usual practice. In view of their report, the Supreme Court did not find it proper to take any legal action against the physician of the nursing home. But the judges observed that initially the patient was treated by a doctor who, despite not having the requisite qualification, administered allopathic medicines to him. Therefore he was a quack. Condition of the patient was “damaged to an unascertainable extent” by his treatment before the patient was shifted to the nursing home. They found Dr Ashwin Patel guilty and ordered him to pay Rs 3,000,00/ to Mrs Verma as compensation and also Rs 10,000/ as the cost of the process of appeal. A copy of the judgment was also sent to the Medical Council of India to examine the feasibility of initiating legal action against Dr Patel for practicing allopathy without being qualified and registered in allopathic medicines. 2.2.2 Some other cases In 2001, the right to practice allopathy was denied to the diploma holders in nature care and hygiene and also to a doctor qualified in any of the branch of the system of Indian Medicine (Ashtang Ayurveda, Siddha, or Unani Tibb) in the judgments of two separate cases filed at the Gujarat High Court and Allahabad High Court. Again in April 2016, in response to a Public Interest Litigation filed by the Delhi Medical Association (an organization of allopathic doctors), the Delhi High Court held that no practitioner of Indian System of Medicine or integrated medicine would be entitled to practice allopathic medicines.
In 2013, a homeopath practicing at the Bedia village near Rajkot (Gujarat) treated a child with paracetamol and subsequently put him on saline drip. The condition of the child deteriorated further and his father had to approach allopaths. Later on, he lodged a case against the homeopath and got Rs 2,00,000/ as compensation, ordered by a consumer court. In its judgment, the court quoted the judgment of the aforementioned case of the Supreme Court (1996) “A person who does not have knowledge of a particular system of medicine but practices in that system is a quack and a mere pretender to medical knowledge or skill, or to put it differently, a Charlatan”.
In 2016, a homeopath at Dakor (Gujarat) treated a woman (65 years) with some allopathic medicines (including an intramuscular injection) for psoriasis. She developed muscular dystrophy and ultimately had to resort to allopathic treatment. The members of her family lodged a case against the homeopath, who had to agree for an outside the court settlement, paying Rs 2,00,000/ to the patient.
2.2.3 Exceptions associated with the rule
In January 2014 the Maharashtra government announced that the qualified homeopaths could practice some form of allopathic medicine after taking a one-year course at the Maharashtra University of Health Sciences. The government sought to justify the decision citing acute shortage of qualified medical personnel in the rural areas in the state. The Indian Medical Association (IMA) lodged a protest with the logic that the one-year course won’t be sufficient to train the homeopaths in the practice of allopathic medicines. The IMA approached the High Court and subsequently the Supreme Court for an injunction, which would debar the homeopaths from practicing allopathy. The apex court rejected the petition (much to the chagrin of the IMA) on the ground that since 1992, ayurvedic doctors were permitted to practice allopathy in Maharashtra and hence homeopaths could not be stopped from doing so especially in view of the acute crisis caused by the shortage of qualified doctors in the state.
The judgments of the Supreme Court in the aforementioned case (1996) and this case, though appearing to be contradictory, are based on the framework of the law of the land, which keeps healthcare-related issues within the purview of the state governments. According to the section 2(ee)(iii) of the Drugs and Cosmetics Rule 1995, the ayurvedic, unani, siddha and homeopathic doctors are allowed to prescribe allopathic medicines in states, where the state governments have authorized them for this purpose by a general or special order. Interested readers are referred to the judgment of three such cases [Dr. Mukhtiar Chand and Ors. vs. State of Punjab and Ors. (1998); Tamil Nadu Siddha Medical Graduates Association Vs Smt. Letika Saran (2010) ; Dr. J.Santhosh Kumar vs. The Block Medical Officer (2012)].
2.3 Proposal for a bridge course
A proposal was raised in the National Medical Commission Bill (2017) to start a bridge course for the practitioners of alternative medicines (homeopathy and ayurveda) so as to enable them in using some allopathic medicines. As expected, the proposal was strongly criticized by the allopathic doctors. A nation-wide one-day strike was called against the proposal on 1 January 2017. The strike was called off after the bill was referred to the Parliamentary Standing Committee. The bill was opposed by some other quarters also. The Parliamentary Panel for Health, which was reviewing the bill, wanted the government to scrap the proposal for the Bridge Course. Expressing disapproval for crosspathy, one of the members apprehended that it would cause “great harm to ayurvedic medicine “as its practitioners would leave the traditional systems and start practicing allopathy, which is more lucrative. On the other hand, a homeopath defended the proposal on the ground that if homeopaths were allowed to take the Bridge Course it would help to “ease the burden on overworked allopathic doctors and to share the disease burden of the nation”. Even a visionary academic person like Professor Yash Paul proposed for an integrated course, which would include 4-5 commonly used drugs described in different pharmacopoeia. He also proposed for an 8-12 weeks of training or posting for doctors of a particular system of medicine in some other system of clinical practice (e.g, allopaths should be trained in ayurveda and so on). On the other hand some allopaths strongly believe that legalization of crosspathy (which is a shortcut, short-sighted and sightless policy, as viewed by them), will only help to compound and complicate the medical problems.
3. Concluding remarks
Both the problems dealt with in this article, appear to concur at a point (e.g shortage of qualified doctors) as the root cause. But that remains a disputed issue as discussed in Section 1.1.4.1. It is also obvious from the forgoing discussion that it is really difficult to formulate a policy that will ensure safety of the patients as well as availability of medical care even to the people of the remotest villages. It is revealing that even in the developed countries, the policy-makers have come to terms with the reality that effective management of the healthcare system may not be possible only with the help of qualified medical personnel and some amount of deregulation of the right to see patients and prescribe drugs may be inevitable for this purpose (Section 1.1.4). So instead of maintaining a sacrosanct attitude about the medical degree in one hand and throwing the door wide open for the untrained quacks on the other hand, let us think of the alternatives which are working well in other countries.
As to crosspathy, the apprehension that if given liberty, many of the homeopaths and ayurvedic doctors will start practicing allopathic medicine cannot be ignored. The scope of the proposed Bridge Course to train the ayurvedic and/or homeopathic doctors in allopathic medicines within a short time also remains questionable. It will be unwise not to utilize the vast resource of phytomedicines, which are traditionally used in this country in the healthcare management. So the tendency of integrating herbal therapy with modern scientific system of therapeutics appears to be justified. But the idea of many allopaths that use of ayurvedic medicine does not require any training and so they can freely prescribe ayurvedic medicines only on the basis of the reputation of the manufacturers, smacks oversimplification. Plants contain some chemicals with medicinal properties and also some chemicals with potentially toxic properties. Reports on toxicity of herbal medicines abound in the literature. Hence, if any plant product is to be used for therapy, it must be thoroughly studied as to its contents, their effects and side-effects. Moreover it must be borne in mind that simultaneous use of allopathic and plant medicines may be associated with the danger of interaction between the contents of the two types of medicines. It is an issue of serious concern in some Western countries where plant medicines are gaining entry into the market and selling freely as food supplements. Practitioners of allopathic medicines therefore must be well-aware of various types of drug-herb interactions. A plethora of information on this aspect is available online.
References 1) Watson DE, McGrail KM (2009) More doctors or better care? Health Policy Vol 5 (Aug), pp: 26-32.
2) Deo MG (2013) Doctor :Population ratio for India; the reality. Indian Journal of Medical Research.Vol 137(4), pp : 632-635.
3) Kumar R, Pal R (2018) India achieves WHO recommended doctor population ratio: A call for paradigm shift in public health discourse ! Journal of Family Medicine and Primary Care. Vol 7 (5), pp :841-844.
4) Das J, Chowdhury A, Hussum R, Banerjee AV (2016) The impact of training informal health care providers in India : A randomized controlled trial. Science Vol 364 (6308) pii: aaf7384.
5) Verma U, Sharma R, Gupta P, Gupta S, Kapoor B (2007) Allopathic vs ayurvedic practices in tertiary care institutes of urban north India. Indian Journal of Pharmacology Vol 39 (1), pp:52-54.
6) Paul Y, Tiwari s (2014) Issues to settle-Cross system medical practice. Journal of the Association of Physicians of India. Vol 82 (Mar), pp : 244-247.
7) Bada Math S, Moirangthem S, Naveen Kumar C (2015) Public health perspectives in cross system practice: past, present and future. Indian Journal of Medical Ethics. Vol XII (3) , pp 131-136.
8) Kumar R, Roy P (2016) Deregulation of allopathic prescription and medical practice in India: Benefits and pitfalls. Journal of Family Medicine and Primary Care. Vol 5 (2) pp:215-219.
The author (an M.Pharm, Ph.D from the Jadavpur University, Kolkata) is a microbiologist, retired from service at the Centre for Cellular and Molecular Biology (CSIR-CCMB), Hyderabad in April 2016. He also worked for some time at the Inst. Jacques Monod, Paris University (France) and Leibniz Institute for Freshwater Ecology and Inland Fisheries, Neuglobsow (Germany) as a Post-Doctoral Fellow and Visiting Scientist, respectively. He is actively involved in public understanding of science for more than 10 years. He can be reached at madhab.ccmb@gmail.com

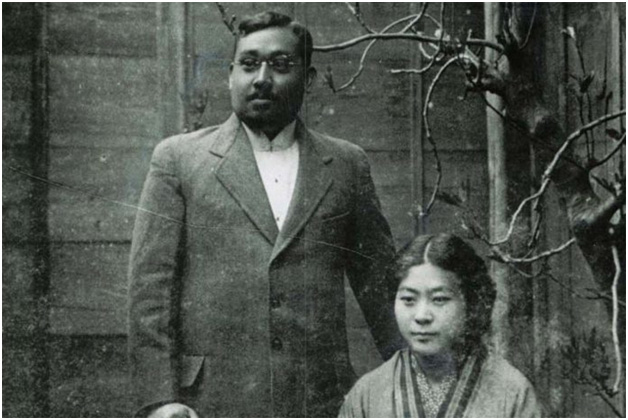
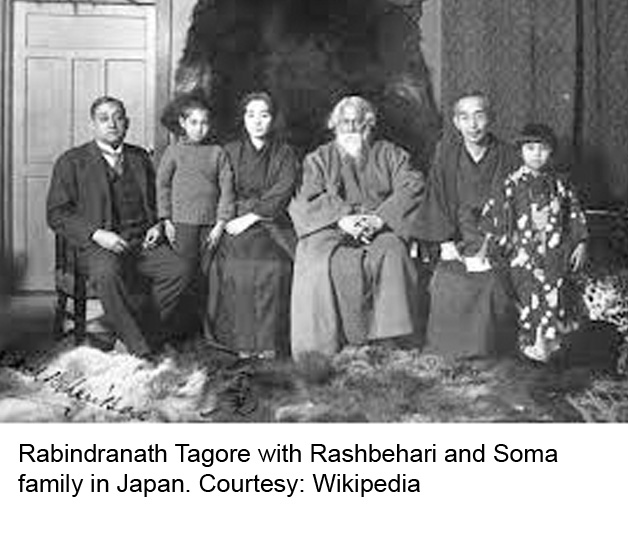
 While studying in Dupleix College in Chandannagar Bose came in contact with the Charu Chandra Roy who was the principal of the college. Charu Chandra inspired the young Bose with the spirit of love for the nation. He realized that independence from an oppressive brutal ruthless foreign regime was the only path that had to be adopted and for that extreme sacrifice is needed. The ground was fertile and the seeds were sown. Now Bose, who was more inclined towards a military career but never got a chance, being a Bengali, had to take up a Government job as a means of livelihood and was staying in Himalayan foothills of the North. However he was influenced and inspired by Aurobindo Ghose and Jatindranath Bannerjee, and secretly worked under the guidance of the latter. He came into prominence through the famous incidence where a major conspiracy was hatched to kill Hardinge, the newly appointed viceroy after transferring the capital of British India from Calcutta to Delhi.
While studying in Dupleix College in Chandannagar Bose came in contact with the Charu Chandra Roy who was the principal of the college. Charu Chandra inspired the young Bose with the spirit of love for the nation. He realized that independence from an oppressive brutal ruthless foreign regime was the only path that had to be adopted and for that extreme sacrifice is needed. The ground was fertile and the seeds were sown. Now Bose, who was more inclined towards a military career but never got a chance, being a Bengali, had to take up a Government job as a means of livelihood and was staying in Himalayan foothills of the North. However he was influenced and inspired by Aurobindo Ghose and Jatindranath Bannerjee, and secretly worked under the guidance of the latter. He came into prominence through the famous incidence where a major conspiracy was hatched to kill Hardinge, the newly appointed viceroy after transferring the capital of British India from Calcutta to Delhi.